10 June, 2026
10 June, 2026Fine Lines on Your Teeth: Are They Enamel Craze Lines?
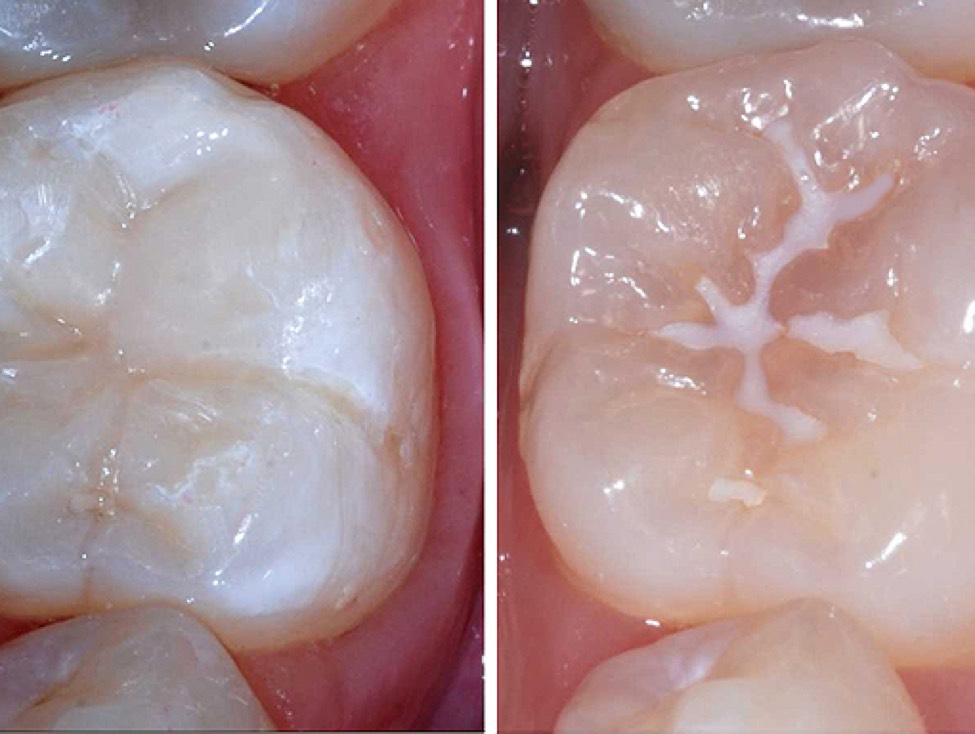
When looking in the mirror or taking close-up photographs, many people are surprised to notice thin, hairline-like lines running vertically along the surface of their teeth. In most cases, these lines are painless, not associated with tooth decay, and do not affect chewing function, so they are often ignored.

Taking care of your teeth helps maintain a beautiful smile and proper chewing function – AI-generated illustration.
However, these lines may be a sign of enamel craze lines—a common dental condition that many people are unaware of. Craze lines not only affect the aesthetics of a smile but may also be associated with unfavorable habits such as teeth grinding (bruxism) or prolonged excessive biting forces.
Most enamel craze lines do not cause pulpal symptoms because the cracks do not extend into the dentin or pulp. However, some patients may report mild sensitivity to temperature changes, acidic foods, or mechanical forces, although these symptoms are generally not specific.
Types of Enamel Craze Lines
Enamel craze lines can generally be classified into two main types.
Internal Enamel Craze Lines
These lines originate at the dentinoenamel junction (DEJ) but terminate within the enamel layer without reaching the enamel surface. As a result, no detectable step or ridge is typically felt during examination with a dental explorer.
Typical Enamel Craze Lines
These lines also originate at the dentinoenamel junction but extend all the way to the enamel surface, making them more readily visible during clinical examination.
Causes and Risk Factors
The exact mechanism behind the development of enamel craze lines has not been fully established. Physical and chemical factors such as repeated mechanical forces, temperature fluctuations, humidity changes, and variations in oral pH may compromise the structural integrity of enamel, leading to the formation of microscopic cracks.
Craze lines are more commonly found in anterior teeth, particularly canines and lateral incisors. Their prevalence varies among studies and age groups, generally ranging from 20% to 50%, and may be even higher in certain populations. Enamel craze lines are most commonly observed in individuals aged 20 years and older.
Risk factors include:
- Teeth grinding (bruxism)
- Clenching habits
- Aging
- Dental caries
- Tooth wear
- Cervical tooth lesions
- Previous dental restorations
- History of orthodontic bracket removal
Among these, bruxism is considered one of the most common contributing factors. The repetitive forces generated during grinding can gradually weaken enamel and lead to the development of fine cracks on the tooth surface.
Diagnosis of Enamel Craze Lines
Diagnosing enamel craze lines requires both clinical examination and imaging support because very fine cracks can easily be overlooked when viewed with the naked eye.
Traditional diagnostic methods may miss extremely small craze lines or fail to distinguish them from other dental defects. Therefore, additional diagnostic techniques are often necessary.
A key aspect of diagnosis is differentiating enamel craze lines from cracks that extend into the dentin. Once a crack reaches the dentin, both prognosis and treatment planning change significantly.
Transillumination Technique
Transillumination is one of the most useful methods for distinguishing these conditions.
When fiber-optic light is directed through a tooth:
- If a crack extends into the dentin, light transmission is interrupted, creating a distinct contrast between illuminated and darkened portions of the tooth.
- If the defect is limited to enamel craze lines, this characteristic interruption of light transmission is generally not observed.
Principles of Managing Enamel Craze Lines
In most cases, enamel craze lines do not require treatment unless they affect aesthetics or produce bothersome symptoms.
In anterior teeth, craze lines may reduce patient confidence, particularly when they become stained, highly visible under certain lighting conditions, or associated with tooth sensitivity.
Therefore, current treatment goals primarily focus on:
- Improving aesthetics
- Preventing discoloration
- Reducing sensitivity when present
- Preserving maximum tooth structure
- Enhancing enamel resistance whenever possible
Within the philosophy of minimally invasive dentistry, conservative approaches should always be considered before restorative treatments such as composite bonding, porcelain veneers, or crowns.
While aesthetic composite restorations, porcelain veneers, and crowns can effectively mask craze lines and improve tooth shape and color, these options are generally reserved for cases involving significant aesthetic concerns, substantial tooth structure loss, or situations where conservative methods have failed to achieve satisfactory results.
Which Treatments Are Most Effective?
Monitoring and Risk Factor Control
For mild craze lines that are asymptomatic and do not affect appearance, periodic monitoring may be sufficient.
Dentists should evaluate:
- Bruxism and clenching habits
- Biting hard objects
- Occlusal trauma
- Tooth wear
- Acidic dietary habits
- Salivary function
For patients with bruxism, nighttime occlusal splints and habit modification may help reduce repetitive forces applied to the enamel.
Enamel Remineralization
Remineralization therapy involves supplying essential minerals to strengthen enamel and support the repair of very early defects.
Commonly discussed materials include:
- Hydroxyapatite
- Nano-hydroxyapatite
- CPP-ACP / CPP-ACPF
- Fluoride
- Supersaturated calcium-phosphate ion solutions
Resin Infiltration
Resin infiltration, particularly the ICON (DMG) system, is a conservative treatment approach that typically requires little to no tooth preparation.
A low-viscosity resin penetrates microscopic enamel defects and fills the craze lines. Once these defects are sealed, differences in light reflection between the craze line and surrounding healthy enamel are reduced, making the lines less noticeable and improving the tooth’s appearance.
Laser-Assisted Remineralization
Dental lasers are being investigated for their ability to modify enamel surfaces and enhance mineral crystallization or deposition, thereby potentially improving remineralization outcomes.
Some researchers have proposed non-invasive treatments using hydroxyapatite or supersaturated calcium-phosphate solutions combined with laser irradiation under safe parameters, without removing tooth structure or damaging healthy enamel.
However, this approach still requires additional clinical evidence. When utilized, lasers should be considered an adjunctive therapy rather than a replacement for accurate diagnosis, occlusal force management, caries prevention, tooth wear control, and appropriate material selection.
Invasive Restorative Treatment
If enamel craze lines are associated with significant discoloration, extensive enamel defects, dental caries, old restorations, loss of tooth structure, or high aesthetic demands, treatment options may include:
- Aesthetic composite restorations
- Porcelain veneers
- Full-coverage crowns
Although these treatments provide excellent cosmetic masking, they require greater intervention to natural tooth structure. Therefore, they should not be considered the first-line treatment for uncomplicated enamel craze lines.
Conclusion
Enamel craze lines are a common condition that is often harmless and primarily affects aesthetics. Accurate diagnosis is essential to distinguish simple enamel craze lines from more serious tooth cracks involving dentin.
In most cases, conservative management—including monitoring, controlling risk factors, remineralization therapies, and resin infiltration—can provide satisfactory outcomes while preserving natural tooth structure. More invasive restorative procedures should be reserved for carefully selected cases where functional or aesthetic concerns warrant additional intervention.
Source: Adapted from an article originally published by Tuoi Tre Online.