12 June, 2026
12 June, 2026Symptomatic irreversible pulpitis is one of the most common causes of acute dental pain in clinical practice. The pain is often spontaneous, prolonged, worsens at night, and can significantly affect a patient’s daily activities, psychological well-being, and quality of life. In most cases, patients seek dental care primarily because of pain; therefore, pain relief remains the highest priority in the management of symptomatic irreversible pulpitis.

Source: Internet
I. PAIN MECHANISM
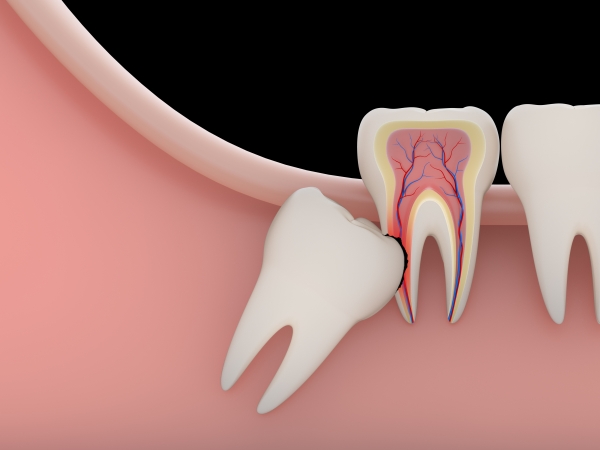
Pain associated with symptomatic irreversible pulpitis originates from the unique anatomical and physiological characteristics of the dental pulp. The pulp is enclosed within a rigid chamber with very limited capacity for expansion. As inflammation progresses, vasodilation and inflammatory exudate accumulation increase intrapulpal pressure, compressing nerve endings within the pulp tissue. Simultaneously, inflammatory mediators such as prostaglandins, bradykinin, and histamine are released, stimulating A-delta and C nerve fibers, resulting in sharp pain upon stimulation as well as dull, spontaneous, and persistent pain.
II. GENERAL PRINCIPLES OF PAIN MANAGEMENT IN SYMPTOMATIC IRREVERSIBLE PULPITIS
Effective pain control in symptomatic irreversible pulpitis cannot be achieved through systemic analgesics alone without addressing the underlying cause. The fundamental principle is to reduce intrapulpal pressure and control inflammation. Treatment should be individualized based on the condition of the tooth, the severity of inflammation, the patient’s general health, and their level of cooperation. Proper mechanical interventions and evidence-based endodontic procedures play a crucial role in pain management.
III. PAIN MANAGEMENT STRATEGIES FOR SYMPTOMATIC IRREVERSIBLE PULPITIS
3.1. Non-Pharmacological Pain Management
Proper access cavity preparation is an essential step in relieving intrapulpal pressure and reducing stimulation of nerve endings. Removal of carious tissue and inflamed pulp tissue, combined with effective rubber dam isolation, irrigation, and temporary sealing, helps prevent reinfection and recurrence of pain. In many cases of symptomatic irreversible pulpitis, decompression of the pulp chamber alone can provide significant pain relief.
3.2. Pharmacological Pain Management
Paracetamol (acetaminophen) and nonsteroidal anti-inflammatory drugs (NSAIDs) are commonly used as adjuncts for pain control in symptomatic irreversible pulpitis. Combination therapy may be considered when enhanced analgesic effects are required. Antibiotics are not routinely indicated and should only be prescribed when there is evidence of spreading infection or systemic involvement.
3.3. Endodontic Intervention for Pain Relief
Endodontic treatment is the definitive method for controlling pain in symptomatic irreversible pulpitis. The procedure includes appropriate local anesthesia, rubber dam isolation, access cavity preparation, cleaning and shaping of the root canal system, placement of intracanal medicaments such as calcium hydroxide when indicated, and temporary restoration. In certain situations, treatment may be completed over multiple visits to ensure patient comfort and safety. For suitable cases, complete pulpectomy and root canal obturation may be performed in a single appointment.
IV. PAIN MANAGEMENT IN SPECIAL CLINICAL SITUATIONS
4.1. Patients with Local Anesthetic Allergy
When a true allergy to local anesthetics is confirmed, clinicians should identify the specific agent involved, such as topical anesthetics, lidocaine, or articaine. Allergy testing may be performed to determine a safe alternative. If local anesthesia cannot be administered, pain relief may be achieved through gentle mechanical decompression of the pulp chamber while avoiding deep instrumentation of vital pulp tissue, combined with systemic analgesics, particularly NSAIDs, or, when necessary, treatment under general anesthesia.
4.2. Uncooperative Pediatric Patients
Managing pain in uncooperative children presents a significant clinical challenge. The primary goal is rapid pain relief while minimizing psychological trauma. The use of arsenic compounds or formocresol for pulp devitalization carries considerable risks, including dosage control issues, accidental ingestion, soft tissue necrosis, and damage to surrounding bone. Therefore, a safer approach involves local anesthesia, rapid access cavity preparation, and the use of biocompatible materials such as chlorhexidine, sterile cotton pellets, or calcium hydroxide, followed by temporary sealing and appropriate behavior management techniques. In particularly difficult cases, treatment under general anesthesia may be considered.
4.3. Pregnant Patients with Symptomatic Irreversible Pulpitis
Acute pain caused by symptomatic irreversible pulpitis is not a reason to postpone treatment during pregnancy. On the contrary, persistent pain may negatively affect both maternal and fetal health. The treatment objective is to safely relieve pain and control inflammation through necessary procedures such as pulp chamber decompression and root canal debridement. Definitive treatment may be postponed until after delivery if appropriate. Paracetamol is generally considered the preferred analgesic during pregnancy.
V. AVOID THE USE OF ARSENIC AND FORMOCRESOL IN THE MANAGEMENT OF SYMPTOMATIC IRREVERSIBLE PULPITIS
Approximately 90% of pain relief in symptomatic irreversible pulpitis results from proper mechanical management rather than from pulp-devitalizing agents. Historically, arsenic compounds and formocresol were used to devitalize the pulp and achieve rapid pain reduction. However, these materials possess significant toxicity, may cause necrosis of surrounding tissues, and offer poor control over the extent of their effects. Consequently, they are no longer recommended in modern dental practice. Timely pulp decompression, staged endodontic treatment, and the use of biocompatible materials such as calcium hydroxide provide comparable pain relief with a substantially improved safety profile.
VI. CONCLUSION
Pain management in symptomatic irreversible pulpitis requires a comprehensive treatment approach based on a clear understanding of disease pathophysiology, adherence to sound clinical principles, and selection of appropriate treatment modalities for each patient. Effective pain control is achieved not by rapidly devitalizing the pulp with toxic substances, but by reducing intrapulpal pressure and managing inflamed tissues through safe, evidence-based, and conservative treatment strategies.
Nhu Ngoc Dental Clinic