11 June, 2026
11 June, 2026Enamel Crazing: Identifying Tiny Hairline Cracks on the Surface of Your Teeth
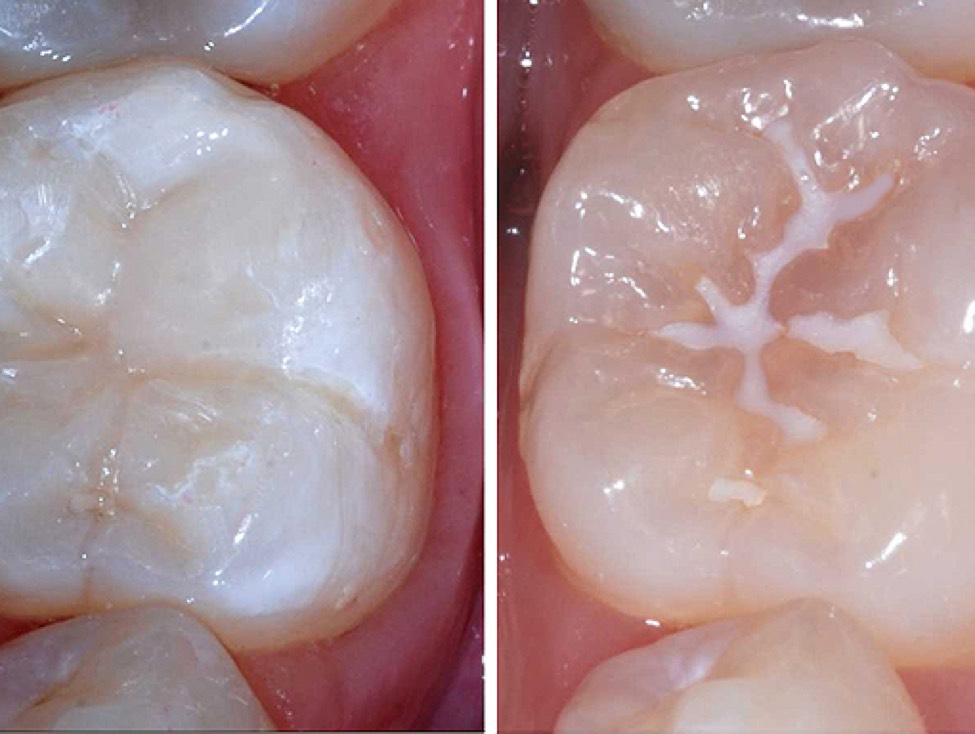
When looking in the mirror or taking a close-up photograph, many people are surprised to discover hairline fractures running vertically down the surface of their teeth. In the vast majority of cases, these lines cause no pain, involve no active decay, and do not hinder normal chewing, which is why they are frequently overlooked.

Proper dental care enhances your smile and secures optimal chewing function – AI Illustrated.
However, these lines can be a primary indicator of enamel crazing (enamel craze lines)—a very common yet relatively unknown type of dental lesion. Enamel craze lines do not just compromise smile aesthetics; they are often linked to adverse habits such as bruxism (teeth grinding) or long-term occlusal overloading (excessive biting forces).
Most cases of enamel crazing are completely asymptomatic because the fracture line does not communicate with the underlying dentin or dental pulp. Nevertheless, some patients may complain of mild tooth sensitivity when stimulated by thermal changes, acidic foods, or mechanical forces, although these symptoms are not highly specific to the condition.
Classification of Enamel Craze Lines
Enamel craze lines are classified into two primary types:
-
Intrinsic Craze Lines: These originate at the dentinoenamel junction (DEJ) but terminate within the enamel layer without reaching the outer tooth surface. Consequently, they are difficult to feel as a ledge or ridge during a clinical examination using a dental explorer.
-
Typical Craze Lines: These originate at the dentinoenamel junction (DEJ) and extend all the way to the outer surface of the enamel, making them much more visible during routine clinical observations.
Causes and Risk Factors
The exact mechanism behind the formation of enamel craze lines remains incompletely understood. However, physical and chemical variables—such as repetitive mechanical stress, sudden temperature fluctuations, moisture variations, and pH shifts within the oral cavity—can degrade enamel integrity, leading to micro-fractures.
Craze lines show a higher propensity to occur in anterior (front) teeth, particularly the canines and lateral incisors. The prevalence of enamel crazing varies across studies and age groups, ranging from roughly 20% to 50%, and can be higher in specific sample populations. It is most commonly detected in individuals aged 20 and older.
The primary risk factors include:
-
Bruxism (nocturnal teeth grinding) and daytime teeth clenching
-
Advanced age
-
Active dental caries (decay)
-
Attrition and erosion (tooth wear)
-
Non-cleft cervical lesions (cervical abfraction)
-
Pre-existing dental restorations
-
Post-orthodontic debonding (removal of braces)
Among these, bruxism is the most prevalent culprit. The repetitive, heavy forces generated during grinding gradually weaken the structural integrity of the enamel, causing these micro-cracks to appear over time.
Clinical Diagnosis
Diagnosing enamel craze lines relies heavily on clinical evaluation and advanced diagnostic imaging, as these tiny lines are easily missed by the naked eye. Traditional examination methods can overlook microscopic lines or fail to differentiate them from other tooth structural defects, requiring a combination of supportive diagnostic techniques.
Crucially, clinicians must differentiate simple enamel craze lines from cracked teeth that have extended deep into the dentin. If a crack propagates into the dentin, the clinical prognosis and treatment plan change completely.
The fiber-optic transillumination (FOTI) technique is highly effective at distinguishing between the two conditions:
-
Cracked Tooth: When a fiber-optic light is placed directly against the tooth, a crack that has penetrated the dentin will disrupt the light transmission, creating a distinct visual boundary where one section of the tooth appears bright and the adjacent section appears dark.
-
Enamel Craze Line: If the defect is restricted entirely to the enamel, this severe light-blocking phenomenon typically does not occur, and the light passes through smoothly.
Principles of Managing Enamel Crazing
Enamel craze lines generally do not require active clinical intervention unless they cause cosmetic dissatisfaction or trigger adverse symptoms. In the anterior region, these lines can cause patients to lose confidence, especially if the cracks become stained, are highly visible under direct light, or are accompanied by localized sensitivity.
Therefore, current treatment objectives focus primarily on:
-
Improving smile aesthetics and removing stains
-
Sealing the cracks to prevent future staining
-
Alleviating hypersensitivity (if present)
-
Maximizing the preservation of natural tooth structure
-
Enhancing the structural resistance of the enamel
Under the philosophy of minimally invasive dentistry, conservative therapies should always take priority before jumping to aggressive options like composite fillings, porcelain veneers, or dental crowns. Invasive methods can mask the craze lines and correct tooth morphology or shading, but they should be reserved for severe aesthetic deficits, cases with concurrent tooth structure loss, or when conservative methods fail to deliver adequate results.
What Protocols Deliver Effective Results?
1. Observation and Risk Factor Management
For mild, painless craze lines that do not present cosmetic concerns, routine periodic monitoring is usually sufficient. The dentist should evaluate the patient for underlying habits like grinding, clenching, chewing on hard objects, occlusal trauma, tooth wear, a highly acidic diet, and salivary flow rates. If bruxism is present, a nightguard (occlusal splint) and habit modification are vital to reduce repetitive forces on the enamel.
2. Enamel Remineralization
Remineralization introduces essential minerals back into the enamel matrix to fortify its structure and reverse early structural damage. Frequently utilized materials in clinical practice include:
-
Hydroxyapatite and Nano-hydroxyapatite
-
CPP-ACP / CPP-ACPF (Casein Phosphopeptide-Amorphous Calcium Phosphate)
-
Concentrated Fluorides
-
Supersaturated calcium-phosphate ion solutions
3. Resin Infiltration
Resin infiltration, famously epitomized by systems like ICON (DMG), represents a highly conservative treatment option that requires virtually no tooth preparation or drilling. A highly fluid, low-viscosity resin penetrates deep into the microscopic enamel craze lines to seal them completely. Once the cracks are filled, the difference in refractive index between the craze line and the surrounding healthy enamel is neutralized, causing the crack to visually disappear and significantly boosting aesthetics.
4. Laser-Assisted Remineralization
Dental lasers are showing great promise in modifying the enamel surface to facilitate crystal growth and mineral deposition, thereby maximizing remineralization efficiency. Some researchers advocate for non-invasive protocols combining hydroxyapatite or supersaturated calcium-phosphate solutions with safe laser irradiation parameters—allowing for treatment without any drilling or loss of healthy tooth structure.
Note: This remains an evolving approach that requires more robust clinical evidence. When applied, lasers should be viewed strictly as a supportive tool rather than a substitute for an accurate diagnosis, bite load management, decay control, and proper material selection.
5. Invasive Restorative Treatment
If enamel crazing is coupled with severe extrinsic discoloration, massive enamel structural defects, active decay, failing old restorations, missing tooth structure, or high cosmetic demands, advanced restorations may be indicated:
-
Cosmetic composite bonding
-
Porcelain veneers
-
Full-coverage crowns
While this category of treatment offers excellent coverage and aesthetic outcomes, it comes at the cost of irreversibly sacrificing healthy tooth structure. Consequently, it should never be utilized as a first-line treatment for isolated, uncomplicated enamel craze lines.