11 June, 2026
11 June, 2026Root Canal Therapy in Primary Teeth: Why Gutta-Percha is Not Recommended
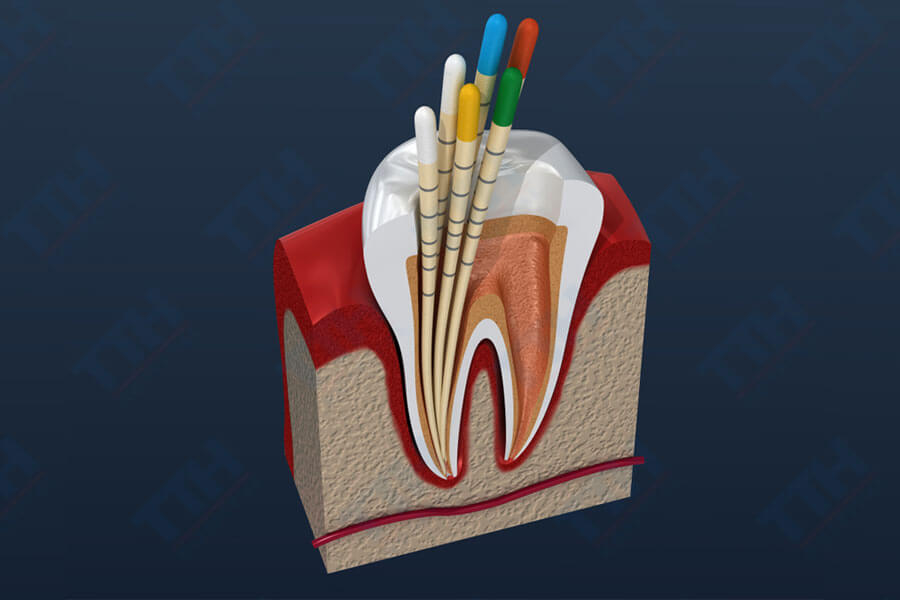
Root canal therapy (pulpectomy) in primary (baby) teeth is a crucial intervention to preserve these teeth until they naturally shed. However, the choice of root canal obturation (filling) material plays a deciding role in the long-term success of the treatment.
While gutta-percha is widely considered the gold standard for endodontic treatment in permanent teeth, it is strictly not recommended for routine use in primary teeth. What is the reason behind this? What clinical consequences can arise if gutta-percha is used in primary teeth?
Why is Gutta-Percha Unsuitable for Primary Teeth?
Unlike permanent teeth, primary teeth possess a unique biological characteristic: their roots gradually undergo physiologic resorption (dissolving) as part of the natural tooth-shedding process. Therefore, an ideal obturation material for primary teeth must be resorbable at a rate close to that of the physiologic root resorption, or at the very least, must not hinder this process.
In contrast, gutta-percha is a highly stable, non-resorbable material that remains virtually unchanged in a biological environment. This fundamental difference creates several clinical risks when applied to primary dentition.
1. Obstruction of Physiologic Root Resorption
One of the most critical consequences of using gutta-percha in primary teeth is its incompatibility with natural root resorption.
When the root of a primary tooth begins to resorb to make way for the erupting permanent successor, the gutta-percha remains intact inside the root canal system or apical region. This disrupts the harmony between the filling material and the body’s natural physiological development.
Potential consequences include:
-
Delayed shedding of the primary tooth.
-
Uneven or asymmetrical root resorption.
-
Prolonged retention of the primary tooth in the dental arch (over-retained primary tooth).
2. Risk of Impacting the Developing Permanent Successor
The goal of root canal therapy in primary teeth is not only to eliminate infection but also to ensure favorable conditions for the permanent teeth to erupt into their correct positions.
When gutta-percha is overextended past the apex or persists long-term in the periapical region, it can:
-
Act as a mechanical barrier along the eruption pathway of the permanent tooth.
-
Cause chronic irritation to the periapical tissue.
-
Increase the risk of disturbing the developing permanent tooth bud.
In certain cases, this can lead to eruption disturbances or ectopic eruption (misaligned direction) of the succeeding permanent tooth.
3. Increased Risk of Persistent Periapical Inflammation
Because gutta-percha is non-resorbable, it remains permanently at the treatment site. If coupled with residual bacterial infection or a prolonged inflammatory response, patients may experience complications such as:
-
Chronic periapical periodontitis.
-
Persistent damage to periapical tissues.
-
Recurrent abscess formation.
-
Prolonged pain or discomfort.
Ultimately, this significantly lowers the long-term success rate of pediatric endodontic treatments.
4. Potential Risk of Radicular Cyst Formation
Some clinical case reports have documented the development of radicular cysts following primary tooth root canal treatments where gutta-percha was used.
While gutta-percha cannot be definitively labeled as the sole cause, the prolonged presence of a non-resorbable foreign material in the apical area is considered a contributing factor that maintains chronic inflammation and prompts cystic lining proliferation. This is a complication that requires vigilant monitoring through routine clinical follow-ups and diagnostic X-rays.
Which Materials are Recommended for Primary Teeth?
Modern pediatric endodontics prioritizes obturation materials that are bio-resorbable or semi-resorbable to match the natural tooth-shedding timeline.
Commonly used materials include:
-
Calcium Hydroxide combined with Iodoform (e.g., Vitapex/Metapex).
-
Modified Zinc Oxide Eugenol (ZOE) pastes.
-
New-generation bioceramic materials.
-
MTA (Mineral Trioxide Aggregate) under specific clinical indications.
These materials are specifically formulated to deliver:
-
✔ High biocompatibility.
-
✔ Support for periapical tissue healing.
-
✔ Zero interference with physiologic root resorption.
-
✔ Minimal risk to the underlying permanent tooth bud.
Are There Any Exceptions Where Gutta-Percha Can Be Used in Primary Teeth?
Though not recommended routinely, gutta-percha may be considered in highly specific, exceptional scenarios. For example:
-
When the primary tooth lacks a succeeding permanent tooth bud (congenitally missing successor).
-
When the long-term clinical goal is to retain the primary tooth in the arch for as long as possible.
However, even in these unique cases, numerous studies indicate that bioceramic materials like MTA yield far superior clinical and radiographic outcomes. Therefore, material selection must be carefully evaluated by a specialist on a case-by-case basis.
Conclusion
Obturating primary root canals with gutta-percha can lead to various adverse outcomes, such as halting natural root resorption, disrupting the eruption of permanent successors, and increasing the risk of chronic periapical lesions.
Consequently, gutta-percha is not considered a preferred choice in the vast majority of pediatric root canal treatments. Utilizing appropriate bio-resorbable materials ensures more effective preservation of primary teeth and safeguards the natural transition to permanent dentition.
At Nhu Ngoc Dental Clinic, every pediatric root canal case is meticulously evaluated based on the child’s age, root integrity, and the developmental stage of the permanent successor to deliver a safe, scientific, and optimal treatment outcome for your child.