11 July, 2026
11 July, 2026
Many people suffer from sleep apnea but are not fully aware of the condition – Illustrative image.
What is Obstructive Sleep Apnea (OSA)?
Obstructive Sleep Apnea (OSA) is a sleep-related breathing disorder characterized by repeated episodes of partial or complete collapse of the upper airway during sleep, resulting in reduced or completely blocked airflow.
Many individuals live with OSA without realizing they have the condition.
When discussing a retruded chin, most people think only of facial aesthetics—a shorter or less prominent chin that affects facial balance. However, in patients with mandibular retrusion, the issue extends far beyond appearance. A retruded lower jaw can significantly impair airway function, particularly during sleep.
In clinical practice, many patients seek medical attention because of loud snoring, restless sleep, or persistent fatigue despite getting a full night’s rest. Comprehensive clinical evaluation combined with diagnostic imaging often reveals that the underlying cause is a retruded mandible, which reduces the space within the upper airway.
For these patients, mandibular advancement surgery not only improves jaw alignment, occlusion, and facial aesthetics but can also enlarge the upper airway. This anatomical improvement may reduce the severity of obstructive sleep apnea, allowing patients to sleep more soundly, wake feeling refreshed, and experience a substantial improvement in their overall quality of life.
Obstructive Sleep Apnea: Understanding a Silent Health Condition
Obstructive Sleep Apnea (OSA) is a sleep-related breathing disorder in which the upper airway repeatedly narrows or collapses during sleep, obstructing normal airflow. As a result, affected individuals experience recurrent episodes of apnea (complete cessation of breathing) or hypopnea (partial reduction in airflow) throughout the night.
Each episode may last from several seconds to more than one minute, leading to decreased blood oxygen levels. In response, the brain briefly arouses the sleeper to restore normal breathing. Because these arousals are usually very short, most patients remain unaware of them until family members notice loud snoring or witnessed breathing pauses during sleep.
Common signs and symptoms of OSA include:
- Persistent loud snoring
- Recurrent pauses in breathing during sleep
- Fragmented or non-restorative sleep
- Frequent nighttime awakenings
- Dry mouth and morning headaches
- Excessive daytime sleepiness
- Poor concentration and memory
- Persistent fatigue despite adequate sleep duration
Without timely diagnosis and treatment, OSA not only compromises sleep quality but also substantially increases the risk of cardiovascular and metabolic diseases, including hypertension, stroke, myocardial infarction, cardiac arrhythmias, and type 2 diabetes mellitus.
Furthermore, excessive daytime sleepiness associated with OSA significantly increases the risk of motor vehicle accidents and occupational injuries, ultimately reducing overall health and quality of life.
Why Does Mandibular Retrusion Increase the Risk of OSA?
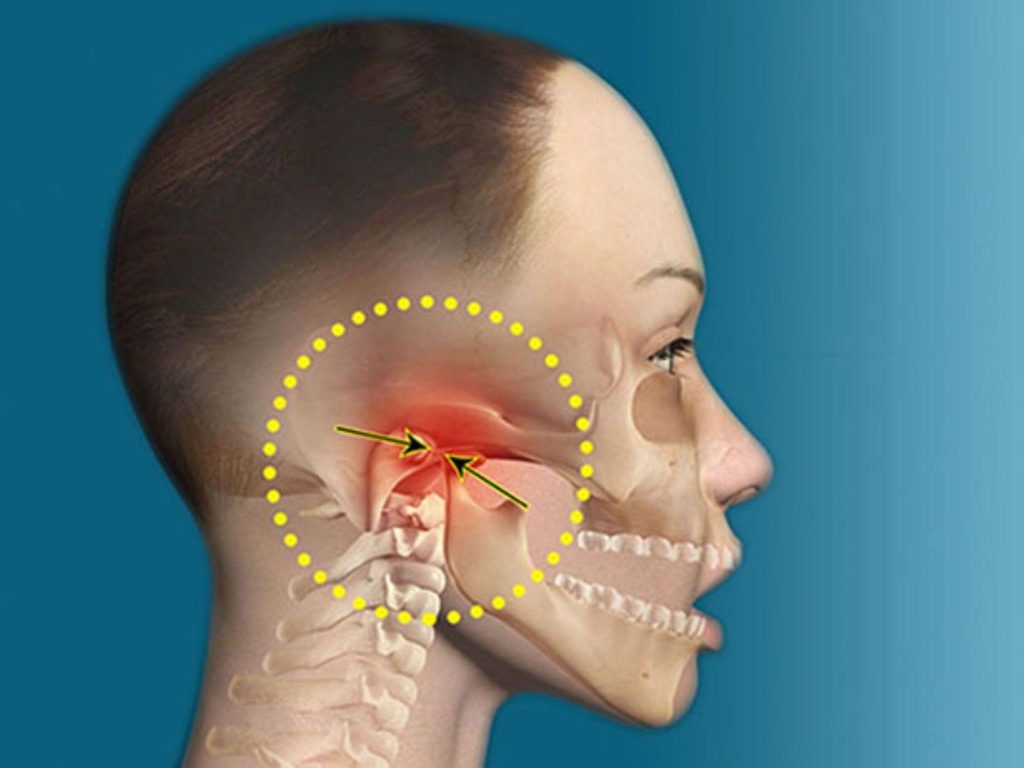
The upper airway can be compared to a flexible tube that must remain open to allow normal airflow. Unlike many other structures in the body, the posterior airway lacks rigid bony support and relies primarily on surrounding soft tissues—including the tongue, soft palate, and pharyngeal muscles—to maintain airway patency.
The mandible serves as the attachment site for several muscles responsible for positioning the tongue forward. When the mandible is retruded, the tongue base and surrounding soft tissues are displaced posteriorly, reducing the airway space, particularly behind the tongue.
While awake, muscle tone within the pharynx is generally sufficient to keep the airway open. During sleep, however, physiological muscle tone naturally decreases. If the airway is already narrowed because of mandibular retrusion, it becomes much more susceptible to collapse during inspiration, leading to obstructive sleep apnea.
For this reason, individuals with craniofacial characteristics such as a retruded chin, mandibular deficiency, or mandibular hypoplasia have a significantly higher risk of developing OSA compared with the general population.

Obesity affects more than 1 billion people worldwide – Photo: Freepik
Not Every Snorer Is Overweight
A common misconception is that obstructive sleep apnea occurs only in overweight or obese individuals. While obesity is indeed one of the strongest risk factors for OSA, it is far from the only cause.
Among Asian populations, including Vietnamese individuals, many patients with a normal Body Mass Index (BMI) are still diagnosed with OSA. In these cases, the primary contributing factor is often craniofacial anatomy rather than excess body weight.
Common anatomical characteristics include:
- Mandibular retrusion
- Underdeveloped lower jaw
- Short or recessed chin
- Narrow upper airway
- Posteriorly positioned tongue base
These structural features increase the likelihood of airway obstruction during sleep, even in individuals who are not overweight.
Therefore, when OSA is primarily caused by craniofacial anatomy, weight reduction—although beneficial for overall health—often does not address the underlying anatomical narrowing of the airway.
Does Every Patient with OSA Require Surgery?
Surgery is not the appropriate treatment for every patient with obstructive sleep apnea. The choice of treatment should be individualized based on the underlying cause of airway obstruction and the patient’s specific clinical characteristics.
When OSA is primarily associated with obesity, enlarged tonsils or adenoids, allergic rhinitis, or other upper airway disorders, management should first focus on treating these contributing conditions before considering surgical intervention.
However, when the primary cause is craniofacial skeletal abnormalities—such as mandibular deficiency, mandibular retrusion, or anatomically narrowed upper airways—orthognathic surgery, particularly mandibular advancement procedures, can provide substantial therapeutic benefits.
By advancing the jaws forward, these procedures enlarge the upper airway, improve airflow during sleep, reduce airway collapse, and significantly alleviate the severity of obstructive sleep apnea in appropriately selected patients.
Source: Tuổi Trẻ Newspaper
Prof. Dr. Võ Trương Như Ngọc